
by Brooke Yang
Illustration: The Soul of the Body by Tiffany Chaey
One of the most morally challenging questions related to medical ethics is whether or not healthcare should be rationed. However, today, as well as throughout the history of medicine, the existence of limited medical resources has deemed the rationing of healthcare necessary and unavoidable. The challenge that arises is in rationing medical resources in a manner that upholds the highest possible standards of medical ethics. Within the category of explicit rationing,1 efforts are made to definitively state rules and guidelines that medical professionals follow in order to make rationing decisions. The topic of organ allocation falls under this category. Organ allocation gives rise to ethical controversies because it is difficult to ethically and fairly utilize the right sets of criteria to determine which patients receive needed organs at a given time and which patients do not. However, an overarching goal in medicine, as well as society in general, is to do what is best for all individuals. Therefore, the ethical allocation of organs, as well as other resources, is a major priority.
In the United States, the Organ Procurement Organization is responsible for taking custody of donated organs and matching organs to patients based on both objective and more subjective medical factors.2 Objective factors include organ type, blood type, and organ size, while subjective factors include level of medical urgency, time on the waiting list, and distance from the donor organ to the patient.3 Computer programs compare these factors to patients’ medical information in order to create a ranked list of patients who should receive each donated organ.3 The United Network for Organ Sharing uses probability of success and time on the waiting list as two of the most important criteria for allocating organs.2,3 These factors are connected to important ethical principles in medicine and society that must be upheld if organ allocation is to be done in a way that truly benefits transplant patients, and therefore is truly ethical. This essay will explore the ethical challenges that probability of success and time on the waiting list present. In addition, this essay will touch upon the importance of considering medical need as a criterion and consider which criteria best account for patients’ well-being.
When probability of success is used as a criterion for allocation, patients that are most likely to succeed medically after receiving a transplant are prioritized in the selection process.2,4,5,6,7 However, simply prioritizing patients who have a higher probability of success from a medical viewpoint fails to establish patient autonomy and respect.2,4,8 At face value, determining a patient’s probability of success is an objective task performed by physicians, in which physicians assess patients’ post-transplant prognosis using objective medical factors8. However, Australia’s National Health and Medical Research Council contends that patients’ probability of success cannot be a purely medical consideration. Instead, it must encompass patients’ emotional and personal values.5 Often times, what doctors define as a medically successful outcome is not what a patient defines as an ideal outcome.2,4,8 For transplant patients, a good outcome does not simply mean gaining a functional organ, but instead means being able to live a healthy and burden-free life. In order to practice ethical medicine, doctors need to consider, for example, how well a patient will be able to participate in their favorite hobbies or how independently a patient will be able to live his or her life.
The lack of independence that patients may experience is an example of the importance of considering the emotional and psychological aspects of recovering and living after an organ transplant. Notably, psychological studies conducted by medical professional Nancy E. Flamme and colleagues show that physicians are less likely than psychosocial evaluators to consider emotional aspects that may affect a patient’s recovery.6 This is concerning because having adequate social support is essential for transplant patients to achieve good health outcomes. Thus, patients’ social support must be evaluated when making organ allocation decisions.6 Psychologist Concetta de Pasquale and colleagues reveal how it is common for transplant recipients to experience anxiety associated with the fear of their body rejecting their new implant, among other health concerns. In addition, “The acceptance of transplant status change is often difficult for family members who have had to redefine roles within the family and recognize the effective autonomy skills of their relative.”9 Family members may face challenges with having to care for their relatives during their recovery, yet family support is essential for post-transplant success. Thus, in evaluating probability of success, physicians must make sure that patients have the necessary family support, as well as other tools such as psychotherapeutic programs to cope with the emotional aspects of recovery.9 In addition, it is important to consider the challenges that patients’ family members face while caring for their loved ones by providing them with necessary resources to provide this care.9
Without considering the psychosocial aspects of a patient’s recovery and life post-transplant, patients’ true medical and emotional needs are not accounted for, which does not accomplish the important medical goal of making patients the center of every medical decision. Relying purely on medical definitions of post-transplant success does not take patients’ holistic well-being into account, so using medical probability of success as an organ allocation criterion is only ethical when it is coupled with consideration for a patient’s emotional well-being.
Another ethical counterargument to the idea of allocating organs based on medical probability of success is that patients with chronic illnesses or poorer overall health are disadvantaged.5 Many proponents of this argument believe that organs should be distributed based on the principles of egalitarianism, meaning everyone should have an equal and fair chance of receiving an organ regardless of their condition.1 All patients who are in need of organ transplants undoubtedly have ill health and believe a transplant could help improve their health. Therefore many people believe that it is unethical to favor certain patients over others based on probability of success.1 Patients with lower probability of medical success post-transplant should have an equal chance at receiving an organ as those with higher probability of success. The principles of egalitarianism support the use of time on the waiting list as the main deciding criterion for organ allocation.1 In fact, waiting time was the main criterion used for allocation of lungs prior to 2005.1
However, numerous ethical issues with relying solely on waiting time have been recognized. The biggest problem is that people forget to consider whether the order of patients on the waiting list actually reflects which patients most need an organ. Admission onto the waiting list can be affected by a patient’s access to quality healthcare.1,6 Bioethics professor James F. Childress explains that patients without health insurance often have to wait to receive care, so they are often not placed on the waiting list as early as possible. However, their health conditions are likely just as serious or more serious than those added to the list earlier.
In addition, a patient’s time on the waiting list can be “easily manipulated.”4 All good doctors seek to cure their patients as quickly as possible. By instinct, physicians with patients experiencing organ failure will attempt to get their patients on the waiting list for an organ immediately.4 This becomes an issue because organs are a limited resource, and if all physicians place their patients on the waiting list as quickly as possible, it is inevitable that some patients with the most urgent medical need for a transplant may remain on the waiting list longer than they should, endangering their health.1,4
When allocating organs only according to waiting list position, the health backgrounds of patients are not accounted for. Similar to relying on probability of success as a criterion, certain patients are disadvantaged in the organ selection process. Probability of success disadvantages those with poorer overall health, while the waiting list disadvantages those with less access to healthcare. In both situations, the patient-centered approach to medicine is not achieved. Both criteria on their own fail to get an accurate view of what patients need in order to achieve a greater level of health.
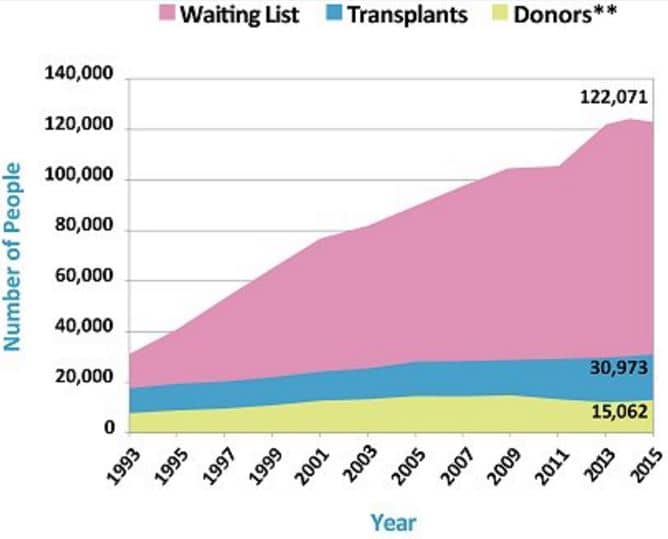
The organ waiting list’s lack of consideration for the true medical need of patients has contributed to the constantly growing number of patients in need of transplants, despite a limited amount of organs. According to the U.S. Government Information on Organ Donation and Transplantation, 22 people die each day while waiting for an organ transplant. At the same time, one patient is added to the organ wait list every 10 minutes.7 Given that such a staggering number of patients die while waiting for a transplant, a patient’s medical urgency for an organ must be considered regardless of his or her position on the waiting list. To rectify this issue, the Department of Health and Human Services proposed the establishment of standard medical measures used to determine a patient’s medical need. All transplant centers are required to follow these guidelines when deciding which patients are medically eligible to be listed for a transplant. Only patients meeting a minimum level of medical need are listed.
In light of the ethical conflicts explored throughout this essay, I think that the most ethical method of organ allocation follows the utilitarianism model for medical rationing, which emphasizes medical need and probability of success as the most important criteria for medical rationing.1 Although there are conflicts over the evaluation of these criteria, these conflicts can be resolved through deliberate efforts to account for patients’ needs. By making the patient the center of every organ allocation decision that is made, the highest possible ethical standards in medicine are achieved despite the inevitable constraints that limited resources present.
References:
[1] Scheunemann LP, White DB. The Ethics and Reality of Rationing in Medicine. Chest. 2011; 140(6): 1625-1632. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3415127/. Accessed December 3, 2015.
[2] Ethics of Organ Transplantation. University of Minnesota’s Center for Bioethics. http://www.ahc.umn.edu/img/assets/26104/Organ_Transplantation.pdf. Published February 2004. Accessed December 3, 2015.
[3] Policy Development. United Network for Organ Sharing. https://www.unos.org/policy/policy-development/. Published 2015. Accessed December 3, 2015.
[4] Childress, JF. Putting Patients First in Organ Allocation: An Ethical Analysis of the U.S. Debate. Cambridge Quarterly of Healthcare Ethics. 2001; 10(4): 365-376. https://www.ncbi.nlm.nih.gov/pubmed/14533403. Accessed December 3, 2015.
[5] Ethical Issues Raised by Allocation of Transplant Resources. National Health and Medical Research Council. https://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/e31.pdf. Published 1997. Accessed December 3, 2015.
[6] Flamme, NE, Terry CL, Helft PR. The Influence of Psychosocial Evaluation on Candidacy for Liver Transplantation. Progress in Transplantation. 2008; 18(2): 89-96. http://pit.sagepub.com/content/18/2/89.abstract. Accessed December 3, 2015.