
by Michael Avgerinos
Mycobacterium avium-intracellulare Complex (MAC) is a nontuberculous mycobacteria (NTM) that causes chronic, debilitating, progressive lung disease in humans. A cousin of Mycobacterium tuberculosis (TB), it typically attacks the lungs, and can become resistant to antibiotics. TB, however, can be cured with six to nine months of treatment with three or more antibiotics. There is no true cure for MAC infections, although the bacteria can be suppressed with a minimum of 12 to 18 months of treatment with at least three antibiotics, whose side effects include hearing loss, vision loss, and kidney and liver toxicity. MAC lung infections, once thought to attack only those with compromised immune systems, is on the rise in immunocompetent individuals, particularly in non-smoking, white, postmenopausal women with no evident risk factors. To prevent progressive lung disease among immunocompetent individuals will require genetics research to determine who may be predisposed to MAC, environmental health research to determine which environmental factors make the human lungs susceptible to these infections, and education to raise awareness among health care providers, health insurers, and the public.
NTM are environmental pathogens that naturally exist in soil and water. People are continually exposed to MAC and other NTM species, but the human immune system typically fights off the bacteria. MAC infection is rare enough that it is considered an orphan disease, and there has not been much interest in researching it. In addition, many primary care physicians, especially in rural areas, are not familiar with NTM infections. Diagnosing MAC infection is difficult, mainly because it is a relatively rare disease and it shares symptoms with common respiratory infections, including fever, cough, night sweats, and fatigue. At a recent FDA Patient-Focused Drug Development Public Meeting on NTM infections, many NTM patients reported recurring bouts of pneumonia, extreme fatigue, and coughing spells severe enough to break one or more ribs (Public Meeting). Many also described feeling ill for several years before a diagnosis was finally made.
The official statement of the American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA) describes clinical and microbiologic criteria required to diagnose NTM lung disease. Clinically, patients should present with pulmonary symptoms, nodular or cavitary opacities on a chest x-ray, or CT scan showing multifocal bronchiectasis with nodules (Griffith ATS). Diagnosis should also include three or more sputum samples or fluid obtained through bronchoscopy that test positive for acid-fast bacteria (AFB).
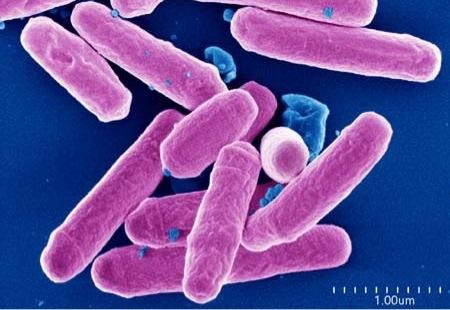
NTM bacteria and TB both become red with acid-fast staining (Fig. 1), but identifying the exact mycobacteria species requires positive culture results. MAC is a slow growing NTM species which takes approximately six weeks to culture. Patients who are suspected of having NTM but do not meet the diagnostic criteria should be followed clinically until diagnosis is made to avoid treating the patient with an antibiotic to which the bacteria are resistant. Patients whose symptoms are severe and cannot wait six weeks for a diagnosis should not be treated with a single macrolide drug to avoid developing resistance.
Treatment for MAC, which comprises the vast majority of NTM cases in the U.S., involves a macrolide (clarithromycin or azithromycin), rifampin, and ethambutol. Blood must be monitored monthly for evidence of liver or kidney toxicity. Monthly sputum samples must be cultured until there are 12 consecutive months of negative sputum cultures. Hearing and vision must be checked periodically for signs of hearing loss and retina damage.
NTM bacteria can cause skin and soft tissue infections, isolated lung disease, or it can cause disseminated disease that can attack any organ in the body. Most NTM infections present themselves as an isolated lung disease, with MAC being the most prevalent NTM species observed (Fig. 5, 6). MAC was first identified in elderly male smokers who had emphysema (Saleeb and Olivier). Research and awareness of clinical syndromes caused by NTM began in the 1980s in response to the AIDS epidemic and the surge in disseminated NTM infections associated with HIV/AIDS. Today, disseminated NTM infections have declined dramatically among HIV populations, owing to the use of antiretroviral drugs that boost the body’s immune system (Daley and Griffith).
In 1997, just 50 species of NTM had been identified, with 13 described as respiratory pathogens. Now, more than 50 NTM species have been identified as respiratory pathogens, thanks to high-performance liquid chromatography and DNA probes (Daley and Griffith). Better laboratory techniques have helped to identify new strains of NTM, although a study of pulmonary NTM in Canada from 1998-2010 concluded that improved laboratory methods did not explain a 40% rise in five-year prevalence rates (Marras et al.).
Pulmonary NTM disease is an epidemiological challenge because it is not spread from person to person, so reporting is not mandatory in most countries, environmental exposure varies widely by geographic region (Fig. 8). NTM colonization may not result in active infection, and the risk factors for the disease are not well understood (Bodle et al.). In order for NTM to attack, an individual must have a predisposition to the pathogen or injury to the lungs that makes the lungs vulnerable to attack, and a direct environmental exposure to MAC (Fig. 9). No one knows exactly what predisposes individuals to MAC, but the surge in pulmonary NTM infections in the 65 to 74-year-old age group in a Medicare study suggests that some change that occurs with age is a predisposing factor.
One study noted that MAC infections are rare in women below age 50 (Mirsaeidi et al.). One reason for the increased susceptibility of postmenopausal women to NTM infections may be related to a drop in estrogen. One study determined that “serum levels of macrophage colony-stimulating factor fall during the first 10 years of menopause, which is restored with hormone replacement” (Mirsaeidi et al.). Macrophages are immune system cells that engulf and destroy invading organisms. The study also found that estrogen protects mice from NTM infections “mainly through augmenting macrophage functions” (Mirsaeidi et al.).
Another predisposing factor for women may be Vitamin D deficiency. Researchers at National Jewish Health (NJH) in Denver note the average pulmonary NTM patient at NJH is a tall, thin, female Caucasian patient in her sixties; black women do not present with pulmonary NTM at all (Huitt). NJH researchers also found that so many NTM patients had consistently low levels of Vitamin D, and since Vitamin D plays a role in the immune system, this may suggest that Vitamin D has a role to play in preventing NTM infection (Huitt).
Vitamin D and calcium are recommended for optimal bone health and fracture risk reduction, and both are essential in any osteoporosis management strategy (Sunyecz). Clearly, more studies need to be done to try to pinpoint why postmenopausal Caucasian women appear to be so disproportionately vulnerable to pulmonary NTM infection. Since NTM does not appear to attack black women at all, perhaps one area of research should be to examine if osteoporosis is a risk factor for NTM disease, especially in view of the fact that black women have higher bone mineral density than white women (Fig. 10).
Bisphosphonate drugs were approved in the 1990s to treat osteopenia and osteoporosis, which is approximately when NTM infection was first identified among immunocompetent Caucasian women. In addition, many women stopped taking hormone replacement drugs in 2002 following negative reports from the National Institutes of Health Women’s Health Initiative study. An examination of data related to hormone replacement therapy or bone density drugs might be instructive in understanding why some women are predisposed to NTM attack.
To understand why immunocompetent non-smokers develop structural lung problems that lead to NTM infections, researchers ought to examine environmental pollutants. Human lungs are particularly vulnerable to injury from particulate matter (PM) in the air, so environmental health research could help to determine if air pollutants contribute to host-risk factors for pulmonary NTM disease. MAC is not a communicable or reportable disease like TB, so there is little data to assist in understanding why so many people are susceptible to it.
Perhaps researchers can investigate data from the WTC Health Program as a proxy database. The 9-11 World Trade Center (WTC) plume contained high pH dust from concrete, gypsum, and glass fibers, which led to respiratory illnesses among thousands of responders, residents and workers near the WTC site (Blanc). There are currently 73,000 people registered in the WTC Health Program, many of whom suffer from various respiratory diseases, such as bronchiectasis and gastroesophageal reflux disease (GERD), which are WTC-related health conditions. That is a statistically significant database with patients who have conditions such as bronchiectasis, GERD, and chronic obstructive pulmonary disease COPD (CDC.gov). Those are the same conditions that are known risk factors for pulmonary NTM infection.
NTM pathogens are everywhere, but environmental research should be done to determine the exact reservoirs, methods of transmission, and portals of entry for human NTM infection. NTM biofilms can live in household plumbing, and NTM have even been found in showerheads (Gorman). Hospitals are also a frequent a source of NTM infection, perhaps because hospitals keep hot water at a temperature that is not sufficient to kill NTM for fear of scalding patients (Thomson).
There is still much to be learned about NTM infections, but the fact that the infection is associated with aging and is now attacking immunocompetent individuals makes it a serious public health threat. As a solution for the long-run, scientists and medical professionals should develop more efficient tests to identify NTM and begin drug trials to help develop more efficient drugs against the infection. The FDA is well aware of the increasing prevalence of various NTM infections, and the fact that the recommended drug regimen is long, costly, and too often results in drug resistance, drug-drug interactions, or drug-related toxicities. The MAC cure rate is at best only 50%, with many researchers arguing that there is really no cure, but instead only suppression of the pathogen. The FDA is currently in the process of soliciting input from NTM patients in its Patient-Focused Drug Development program. In the short-run, the most useful action is a public awareness program to help patients and their primary care physicians identify risk factors for NTM so that a proper diagnosis can be made before an NTM infection has a chance to become resistant to antibiotics and cause irreversible damage to lung function.